Continuing and Chronic Care – comments on your comments
October 28, 2014

Please note: You can now post a comment on this President's Letter without logging in.
Dear Member:
I had an excellent response to my October 10 President’s Letter that dealt with taking action on continuing and chronic care. Thank you to everyone who took the time to write. I was impressed with the thoughtful comments and suggestions.
I thought I would share some of the general themes that appeared in these messages.
- Alberta’s acute care costs
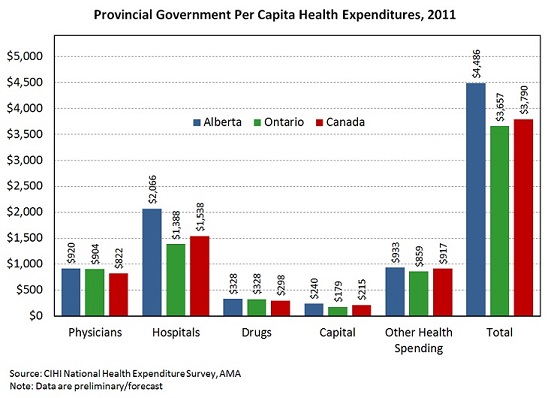
As mentioned in my last letter, Alberta’s acute care costs – particularly hospital costs – are substantially higher than those in other provinces. Alberta’s expenditures in 2011 were $2,066 per capita vs. $1,538 for the rest of Canada.
Members offered thoughts about possible reasons for this significant discrepancy.
- Some suggested that it might be the impact of prices (wages, fees, generally higher costs in Alberta’s economy). Yes, wages are higher in Alberta, but Statistics Canada figures show that average weekly earnings of employees in hospitals were only 6.2% higher than the national average in 2013. (Overall, Alberta average weekly earnings are 21.7% higher than the Canadian average.)
- Others speculated that different provinces might categorize costs differently. That’s possible. For example, if Alberta’s accounting rules place electronic medical record costs within the hospital sector while the other provinces capture them under non-health related categories, there would be a discrepancy.
- Some wondered if we are seeing the impact of Canada’s aging population. Aging accounts for about a 1.1% greater expenditure each year (although about 3% for long term care). In general, Alberta has a younger population than in the rest of the country. We have an influx of young workers and one of the highest birth rates in the country.
- Many have made comments about the apportionment of services. Acute hospital services need to be distributed across the province efficiently, but also in a way that ensures quality and access. It’s not clear if the way Alberta distributes acute care services affects the national comparison of hospital expenditures.
- There were comments about the large number of patients treated in Alberta who come from out-of-province. Certainly we see more transient workers here. (In 2008 there were 13,000 out-of-province resident hospitalizations here vs. 10,000 in the next highest province Ontario.) We also treat residents from rural remote areas in BC and NWT. These expenditures are often recovered through inter-provincial transfers, and those offsets are not accounted for in the provincial expenditure comparisons. Even so, these patients still represent only about 4% of total annual hospitalization in Alberta.
It appears that these factors cannot, on their own, account for the magnitude of our acute sector costs.
My sense is that this is a multi-dimensional problem that will require a variety of solutions. It’s going to be very important that we solve this riddle if we are going to progress to a high quality health care system that is truly sustainable.
We are hearing rumblings about another period of economic uncertainty for the province. If physicians want to advocate for more resources, or resources that should be applied differently, then we’d better be able to explain what’s going on now. There’s a lot of work that needs to be done, but I believe the information is there if we – physicians, Alberta Health and Alberta Health Services – want to find the answers.
There’s one other dimension worth noting, and that’s Alberta’s unique challenge with respect to population growth. In 2014, just over 43,000 people came to the province. The provincial government estimates that over the next 25 years there will be an additional 2.2 million citizens living here. Our issues around costs, access and quality will not be addressed without finding ways to manage this growth. And, solutions will not be found overnight.
- New ideas and efficiencies
A number of the emails I received talked about new ways of doing things. Does everything that occurs in hospital have to occur there? Do we do as much in the community as other jurisdictions do? Are we tracking the right kind of information to be able to see what’s going on? Are we making the right use of teams and other health professionals?
Members spoke of the need to be efficient, yet recognized that efficiency alone is not a panacea. The goal is to do the right things to support Albertans and provide quality and appropriate care.
Chronic disease patients have special needs. This is an area where we can do better. We are working to provide each of these patients with a medical home through primary care networks (PCNs), but PCNs alone won’t get the job done. There are interesting things happening in other countries to support these particular patients. What could we bring to Alberta to make a difference?
The common thread in all the emails I received was that we urgently need to make progress. As I mentioned in my last letter, there’s no shortage of good ideas. We just need to turn some into reality.
I know that we are still left with a lot of questions. Until we have some answers, I think it’s our job to keep asking. I look forward to hearing from you throughout the year as you give this further thought.
Writing this letter coincided with the conclusion of the four by-elections in our province. I would be remiss not to mention the results of yesterday’s votes. Congratulations to Premier Prentice and the winners of all the races. The AMA looks forward to continuing to work with Minister of Health Stephen Mandel under our AMA Agreement.
Email president@albertadoctors.org or leave your comments in the field below.
Regards,
Richard G.R. Johnston, MD, MBA, FRCPC
President
No comments
Commenting on this page is closed.