
Case
Your patient is an 84-year-old man with history of metastatic lung cancer to bone. He presents with severe mid-thoracic back pain from a 50% compression fracture at T9 due to a lytic metastasis. He has been unable to get out of bed because of pain, and has been taking morphine 30 mg q12, plus 10 mg prior to turning, with inadequate relief. You are concerned about pressure sores, thrombosis and pneumonia.
Issue
Pain management in cancer patients with pain refractory to opioids.
Background
The World Health Organization Cancer Pain Ladder was published in 1986 and revised in 1996.1 It still offers a practical approach to pharmacotherapy that has been helpful for millions of cancer patients worldwide.2 It was not designed for use in non-cancer pain or acute pain, but many of its features have been adapted for use in other chronic pain situations. It is important to understand this approach to pain management to know where analgesic procedures might fit in.
The original and revised ladders describe three levels, intended to be used in an escalating manner:
- Step 1 includes non-opioids such as acetaminophen or ibuprofen.
- Step 2 includes “weak” opioids, defined by having a ceiling effect (in Canada primarily codeine and tramadol), or by being attached in fixed combination to a drug that has an upper limit of dose, i.e., acetaminophen. It is now recognized that Step 2 analgesics have inherent risks, and this step is now often appropriately bypassed.3
- Step 3 analgesics are the “strong” opioids that have no inherent dose limit but have widely variable interindividual limits on efficacy. There are risks associated with their consumption, in high doses and in vulnerable patients, for example those with sleep apnea, renal failure, allergy or a substance use disorder. In Canada the most commonly prescribed Step 3 analgesics are morphine, hydromorphone, oxycodone, fentanyl and methadone. Buprenorphine is a more recent addition to this list, and tapentadol is a novel opioid receptor agonist with additional noradrenergic properties.
Choice of drug is only one part of the analgesic ladder. This ladder recommends regular administration rather than as-needed dosing, and encourages the use of longer-acting agents, to allow for sleep and facilitate optimal compliance. It also emphasized concurrent use of “adjuvant” analgesics: those that have effects other than analgesia but provide additional benefit on top of the primary analgesics in some patients. This group includes tricyclic antidepressants, gabapentinoids, corticosteroids, muscle relaxants, cannabinoids and an increasing number of other drugs with unique roles in specific contexts. It is now recognized that sodium channel blockers and ketamine have also been used in particularly challenging situations. They could be considered a second tier of adjuvant analgesics, though are often only considered when Step 3 opioids have been exhausted.
The WHO approach has been applied worldwide for many years and is effective in the majority of patients. However 10-15% of cancer patients do not achieve adequate analgesia with this pharmacologic approach to cancer pain.
Evidence
Though the proportion of cancer patients experiencing drug-resistant pain may seem quite small, even 10% represents a very large number of people. There is also an increasing blurring of the historical separation of cancer vs non-cancer pain. Additionally, there is a rising number of cancer survivors who are living with cancer or side-effects of its treatment for prolonged periods. These individuals suffer greatly, as do their loved ones, and they require immense resources to be cared for. To witness someone with uncontrolled cancer pain leads to fear in those that care for them, professionally or otherwise, such that they may lose faith in the medical system’s ability to relieve their suffering, which is one of the common drivers of requests for Medical Assistance in Dying.
In response to the limits of pharmacological agent alone, a fourth step in the WHO Ladder has been added; that of palliative procedures6 (Fig.1). People living with advanced cancer are frequently too frail for major invasive procedures, hence the need for Minimally Invasive Palliative Procedures, or MIPPs. Examples include:
- Nerve blocks, neurolysis and ablations, including epidural injections and cordotomy.
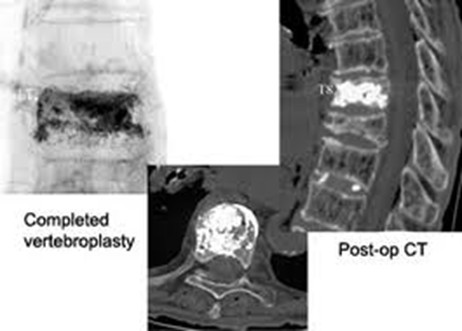
- Bone augmentation with cement, including vertebroplasty, kyphoplasty and pelvic cementoplasty (Fig. 2).
- Tumour ablation for debulking, often combined with cementoplasty
- Embolization for debulking or management of bleeding.
- Neuromodulation via intrathecal infusion or spinal cord stimulation (Figs. 3 and 4).
- Stenting of bowel, blood vessels or other hollow structures.
- Palliative radiotherapy could also be considered a minimally invasive procedure.
MIPPs can be provided by interventional radiologists, anesthetists, neurosurgeons and other specialists with procedural practices, as well as some family doctors who have undertaken extra training in certain procedures, e.g., nerve blocks and epidural injections. The desired effect can sometimes be achieved via more than one approach, and who does it may be determined more by availability than by the most desired method. For example, celiac plexus blocks can be done endoscopically or percutaneously, and peripheral nerve blocks can be done under ultrasound, fluoroscopy or CT scanning, or even without any imaging in an emergency. Procedures requiring higher level skills and specialist equipment include intrathecal infusions with implanted pumps or tunneled catheters and neurosurgical procedures such as cordotomy. Ablation of tissues can be achieved with a variety of devices, including radiofrequency ablation, laser-induced thermotherapy, cryoablation, microwave ablation, and probably other kinds of destructive processes yet to be established. The equipment needed for these needs to be focused in centres where there would be sufficient volume to allow for adequate maintenance of competence by those operating them.
It is difficult to gather data on effectiveness of MIPPs, as they are not a homogenous set of procedures. Also, it would be ethically difficult to randomize a suffering patient to a placebo arm of a clinical trial when there is a plethora of anecdotal data on effectiveness. There are some case series which show excellent results, and some individual procedures often have controlled trial evidence, though the context of the study is important. For example, vertebroplasty for osteoporotic fractures has very different outcomes than from fractures due to malignancy, and data from study of one indication cannot be extrapolated to the other.
Pelvic fractures are an example of where an interventional approach can be transformative for patients. In a British Columbian retrospective study of 48 consecutive cancer patients referred for combination pelvic cryoablation and cementoplasty, there was a 100% technical success rate with no immediate complications. Their average pain scores fell from a mean of 7.9/10 (range: 5 - 10) to a mean of 1.2/10 (range: 0 - 7) the day after the intervention, (P < 0.001), which is clinically very meaningful. The post-intervention pain scores remained stable at 1 to 9 weeks follow-up (mean: 4.1 weeks). Three patients (6.3%) reported no change in pain following the intervention; however, no patients reported worsened pain.7
Another study looked at outcomes from a BC multidisciplinary MIPP case conference8 and showed that of 103 conference referrals, 69 procedures were subsequently performed among 63 patients. The majority of procedures were cementoplasties, nerve blocks and/or epidural injections. Over 80 % of procedures provided analgesic benefit. Pain scores fell across all categories post-procedure. Mean worst pain scores fell from 8.1 ± 1.4 to 4.6 ± 2.8 (P < 0.001). Function, mobility and symptoms measured by the Edmonton Symptom Assessment System also improved. The documented rate of major adverse events attributable to MIPPs was 2/69 (2.9 %).
Despite the evidence of effectiveness and safety of these interventions, there are still many barriers to accessing MIPPs, including the availability of trained staff, the lack of precise criteria, and lack of knowledge of the procedures. Physicians may not know what to ask for, nor who to ask. A multidisciplinary case conference is strongly recommended for discussion of the best procedure for each patient, taking into consideration the clinical and radiological findings, the patient's detailed pain history and psychosocial situation, and the procedures that are accessible to the patient wherever they are.
Summary
Uncontrolled pain can be a medical emergency. We have a moral imperative to do what we can to relieve pain. Palliative procedures should be widely accessible to all cancer patients.
Case Outcome
The patient received a thoracic vertebroplasty and was able to mobilize comfortably before he even left the hospital. Over the next few days, the morphine was tapered to 10 mg q12h with no need for breakthroughs.
Figures


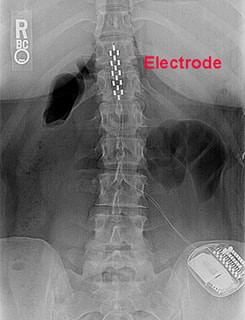
Source: mriquestions.com/spinal-cord-stimulators.html
References
- Ventafridda V, Saita L, Ripamonti C, De Conno F. WHO guidelines for the use of analgesics in cancer pain. Int J Tissue React. 1985;7(1):93-6. [PubMed]
- Stjernswärd J. WHO cancer pain relief programme. Cancer Surv. 1988;7(1):195-208. [PubMed]
- Crush J, Levy N, Knaggs RD, Lobo DN. Misappropriation of the 1986 WHO analgesic ladder: the pitfalls of labelling opioids as weak or strong. Br J Anaesth. 2022 Aug;129(2):137-142. [PubMed]
- Fallon, M. et al. An international, open-label, randomised trial comparing a two-step approach versus the standard three-step approach of the WHO analgesic ladder in patients with cancer. Annals of Oncology, Volume 33, Issue 12, 1296 – 1303
- Pergolizzi J, Raffa R. The WHO Pain Ladder: Do We Need Another Step?. Pract Pain Manag. 2014;14(1).
- Vargas-Schaffer G. Is the WHO analgesic ladder still valid? Twenty-four years of experience. Can Fam Physician. 2010 Jun;56(6):514-7, e202-5. PMID: 20547511; PMCID: PMC2902929.
- Coupal TM, Pennycooke K, Mallinson PI, Ouellette HA, Clarkson PW, Hawley P, Munk PL. The Hopeless Case? Palliative Cryoablation and Cementoplasty Procedures for Palliation of Large Pelvic Bone Metastases. Pain Physician. 2017 Nov;20(7):E1053-E1061. PMID: 29149150.
- Chu L, Hawley P, Munk P, Mallinson P, Clarkson P. Minimally invasive palliative procedures in oncology: a review of a multidisciplinary collaboration. Support Care Cancer. 2015 Jun;23(6):1589-96. doi: 10.1007/s00520-014-2509-4. Epub 2014 Nov 21. PMID: 25412726.
