The Derived Day Approach (DDA) was jointly developed by the Alberta Medical Association (AMA) and Primary and Preventative Health Services (PPHS). It represents a shift in thinking, with a goal to increase fairness across physician compensation models and better align cARP rates with fee-for-service (FFS).
- More transparent and accurate, reflecting current day-to-day clinical practice
- Based on the most recent fiscal year FFS claims data (April to March), with updates every three years, at minimum
- Annualized cARP rates will see an overall increase compared to the historical Provincial Base Payment Rates (PBPR) methodology, with significant increases for some specialties and more modest increases for others
- Family medicine rate for hospitalist programs was effective January 1, 2025 and for programs on April 1, 2025
- On June 25, 2026, specialist rates were announced, retroactive to April 1, 2025
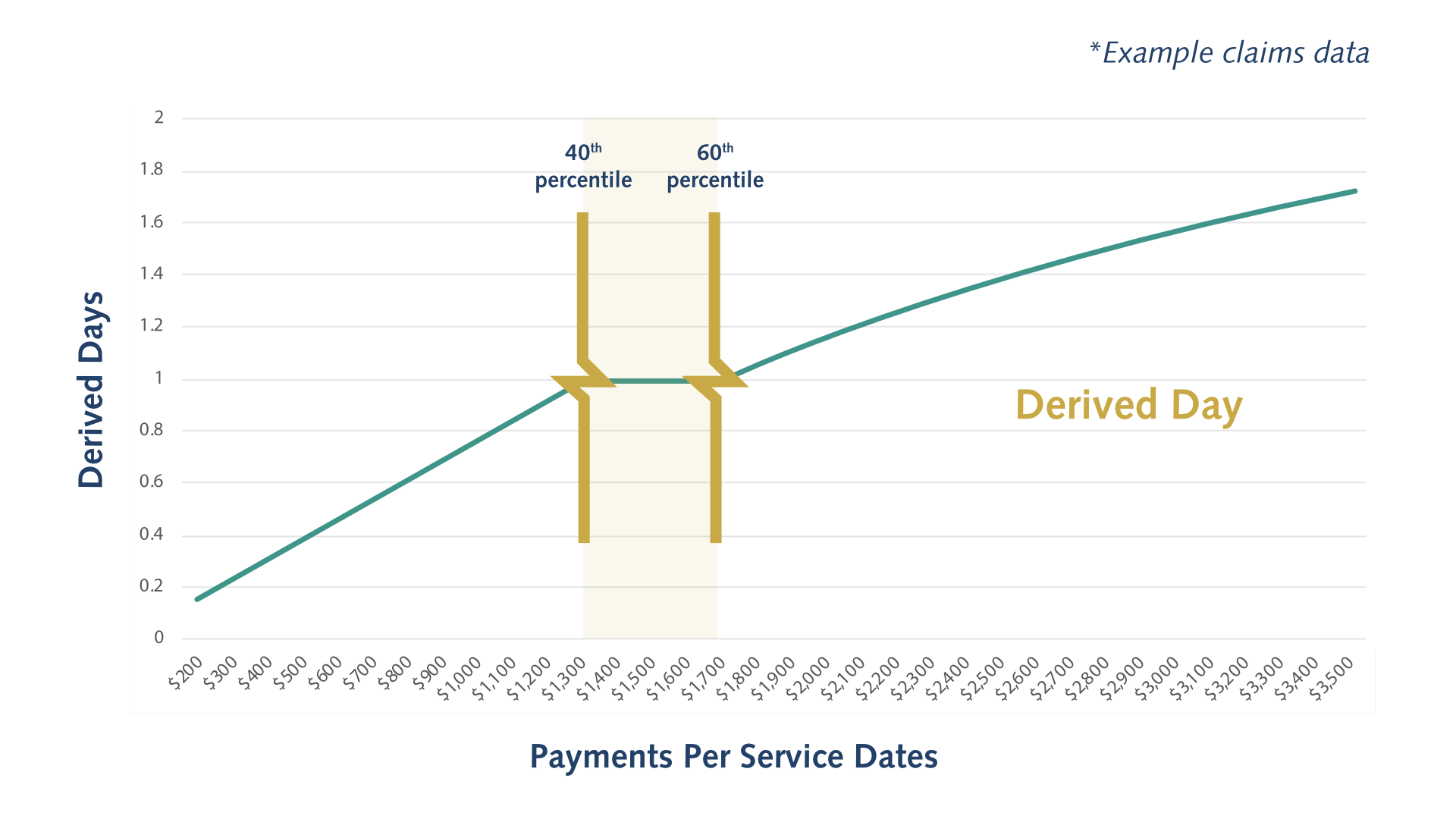
For each specialty or specialty group, the DDA provides an estimate of income earned by a physician on a typical clinical workday, using the 40th-60th percentile of daily FFS billings. This benchmark, known as a Derived Day, serves as a yardstick against which all other days are weighted.
Watch our 3-minute DDA explainer video
DDA Methodology
-
Specialty Section Assignments
FFS claims data and SKILL modifier codes from the most recent fiscal year are used to assign physicians to specialty sections, which are then organized into groups. In some cases, specialties are combined to create more stable and reliable datasets, helping to reduce payment disparities over time.
Group 1: Family Medicine
Group 2: Emergency Medicine
Group 3: Dermatology, Endocrinology & Metabolism, Infectious Diseases, Internal Medicine, Nephrology, Neurology, Pediatrics, Physical Medicine & Rehabilitation, Psychiatry, Respiratory Medicine, Rheumatology
Group 4: Obstetrics and Gynecology, Otolaryngology, Plastic Surgery
Group 5: Anaesthesiology, Critical Care, Gastroenterology, General Surgery, Ophthalmology, Orthopedic Surgery, Urology
Group 6: Cardiology
Group 7: Cardiac Surgery, Neurosurgery, Thoracic Surgery, Vascular Surgery
-
Data Adjustments
During the specialty or specialty group claims data review, non-typical days and non-representative physicians are filtered out. This includes:
- Physicians who bill less than 11 months of the year
- Physicians with annual billings in the top and bottom 5% of their group
- Highly specialized community practice physicians
- Non-FFS shadow billing
- Physicians assigned to surgical sections who don't perform major procedures
- Secondary specialty days with $0 in FFS payments, excluding paediatrics
- Adjustments for cross-over days (shifts that cross over midnight) where 50%+ of a section’s days have TNTP and/or TNTA 03.01AA modifiers - see FAQ for more details
- Non-hospital days with $0 in FFS payments for sections with hospital-based cARPs
Further adjustments take place, including additional data exclusions. For some data points, a separate application of the methodology is applied:
- Weekly patient management fees representing multi-day careare equally distributed across all service days worked per calendar week
- Surgical vs non-surgical days are adjusted to account for bundled payments when a physician in a proceduralist role
- Days where total FFS payments are ≤ 10% of the average payment per service day (net of 03.01AA)
- 03.01AA after-hours time premium payments are excluded
-
Determining a Typical Clinical Workday
Using adjusted FFS billings, a typical clinical workday is established for each specialty or specialty group. Service day values that fall in the 40th-60th percentile of daily billings are considered typical and form what’s known as a Derived Day – the key building block of the methodology.
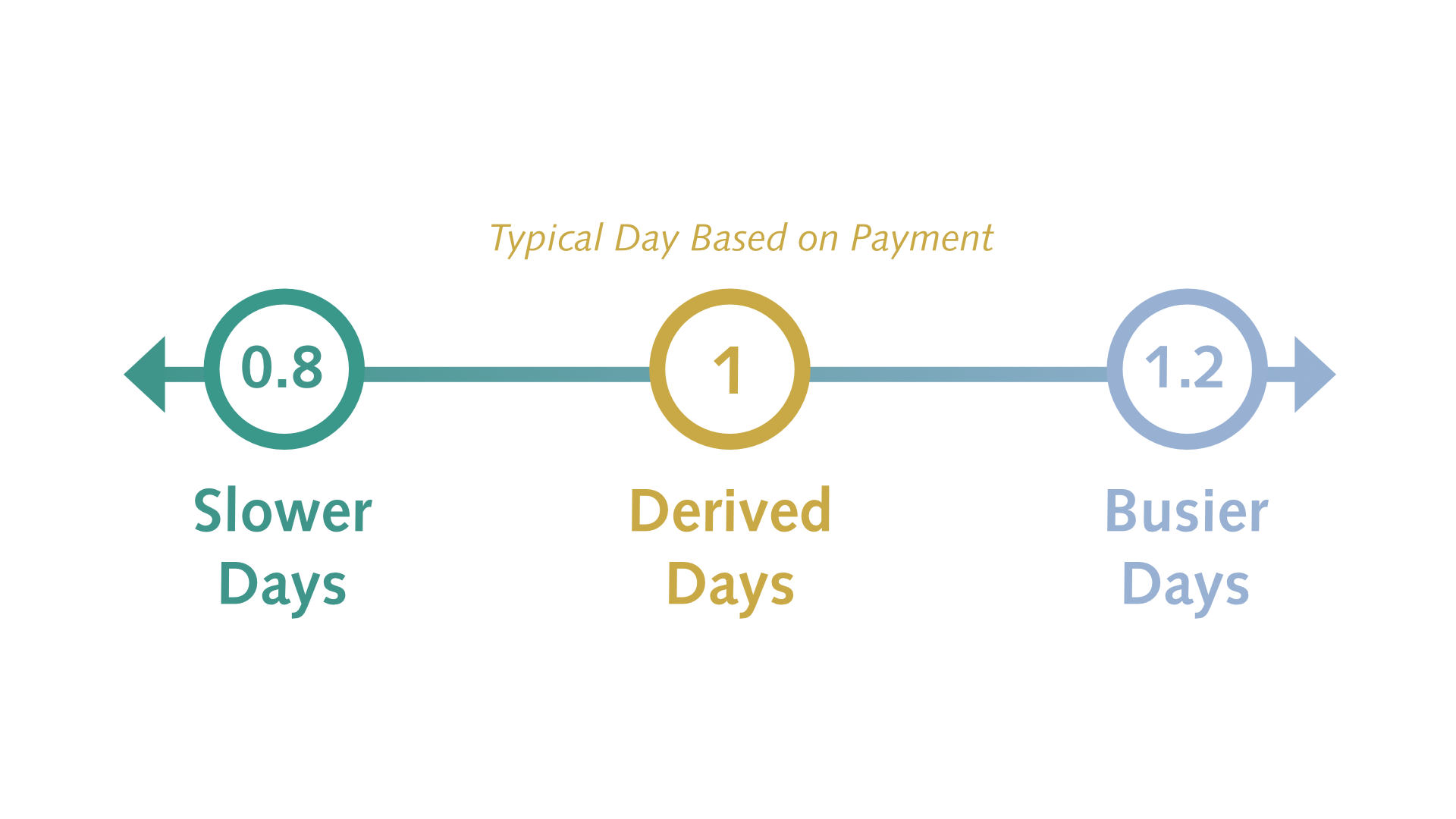
All service days, including outliers, are assigned a Derived Day value:
- Typical days are assigned a value of 1
- Slower days are given a value less than 1, example: 0.8
- Busy days are assigned a value greater than 1, example: 1.2
-
Derived Day Rate (daily cARP rate)
Derived Days worked by each specialty or specialty group are then added together. The total number of days is then divided by the total FFS payments to generate the Derived Day Rate or daily cARP rate, which serves as the base for cARP program funding.

After-hours premium
After-hours time premiums are not included in the base cARP rate calculation. Instead, physicians in eligible programs can bill the 03.01AA premium for regularly scheduled after-hours services with payments provided on top of the base clinical ARP funding.
Future DDA Updates
The DDA reflects the variability of physician practices and is intended to be regularly reviewed and updated through a formal policy, at minimum every three years, in line with:
- Schedule of Medical Benefits (SOMB) changes
- New AMA Agreement
- Non-FFS payments
As funding models evolve, additional elements may need to be integrated into the methodology to ensure fairness and alignment with provincial physician compensation strategies. This may include:
Historical PBPR vs New DDA Approach
|
PBPR |
DDA |
|
|
DDA FAQ
The historical PBPR rate calculation relied on outdated 2002-2003 FFS billing data, adjusted for negotiated rate increases by section, and a CIHI-based FTE approach that produced non-representative rates when a large portion of a section worked part-time.
The DDA will produce more reliable rates and align Annualized cARP compensation with the most current FFS payments. With the DDA, rates better reflect the variability of physician practice patterns and will keep up with changes to SOMB codes and future AMA Agreements.
- Sections with a small number of FFS physicians are grouped with other sections to create more stable and reliable data for rate calculation.
- Specialty grouping provides an immediate solution to physician income equity issues. See next FAQ
- Claims data adjustments and filtering of non-typical days (eg. full-time emergency room physician days working in a walk-in clinic) and non-representative physicians (e.g., part-time physicians) ensure rates are calculated using the most typical clinical day billings. This produces a more reliable, stable dataset that is more accurate and better reflects day-to-day practice. See data adjustments section
- After the daily rate is generated, hourly rates are calculated with standard hours per day for each group. This enables programs to determine the total number of hours or days required to deliver services, providing flexibility and adaptation in establishing program funding for diverse care delivery models. The historical PBPR method relied on rigid FTE definitions; under the DDA, FTE definitions are not assumed.
The DDA is used to set rates in the annualized clinical ARP model, including the clinical component of AMHSPs and does not impact capitation-based ARPs.
Because the DDA is based on current FFS physician data, FFS rate adjustments carry over into cARP rates. Through negotiations and the AMA Agreement, section rate adjustments reflect inflationary adjustments, among other priorities.
FFS rates used in the DDA methodology will be adjusted at least every 3 years, updating group rates for the annualized cARP model over time.
The DDA’s specialty grouping approach provides a mechanism to reduce payment disparities across sections. However, because the methodology uses FFS claims data, underlying income inequities will carry over into cARP rates.
The AMA is preferentially allocating global increases to sections with relatively low-income equity measures through the four-year macro-allocation. As these rate adjustments are implemented, they will help narrow disparities. See June 25 President's Letter
Geographic practice settings are not considered in the current methodology. The DDA is based on the most recent fiscal year FFS claims data, which means underlying inequities will carry over into cARP rates.
Programs may be eligible for the Rural, Remote, Northern Program (RRNP), which can support recruitment and retention challenges.
Elements of complexity are integrated within SOMB codes and modifiers. As such, there is some recognition of complexity in the DDA, as cARP rates are calculated based on FFS physician payments.
The DDA is intended to better align cARP payments with FFS physician compensation. In its design, the DDA will be regularly reviewed and updated. Future changes to the DDA methodology may include ARP payment data alongside other elements.
Rates are based on FFS payments, which are inclusive of overhead. As these costs vary significantly across practices, it is difficult to define or differentiate them within the rate calculations.
Business Cost Program (BCP) funding is available to designated facilities to offset clinic leasing costs and related expenses.
Data Adjustments FAQ
Crossover days are shifts that extend past midnight. In the claims data, a crossover shift is represented as two partial shifts, which can misrepresent daily payments during the claims data review.
Days where only one modifier is used are excluded as they don't represent the entire shift. When consecutive crossover shifts occur and both TNTP and/or TNTA 03.01AA modifiers are billed, the daily payment data is included.
Example: When a physician works three consecutive crossover shifts starting late-night Monday through to early morning on Thursday, claims data for Monday and Thursday are excluded as they don’t represent a full shift. Daily billings on Tuesday and Wednesday include both modifiers, which reflect a typical day for inclusion in the data.
Payment bundling can misrepresent how the data reflects daily payments, so the methodology treats major surgery days separately from non-surgery days. Data adjustments average out larger billing days, so payments are better distributed when deriving daily rates.
DDA Grouping & Rates FAQ
Specialty groupings were implemented to reduce payment disparities. Groupings reflect feedback from specialty sections and consider:
- Similar length of training
- Medical and surgical activities
- Recruitment and retention challenges
The grouping does not factor in job roles or tasks. See next FAQ for details on enhanced skills qualifications within family medicine.
The DDA was designed to accommodate variable schedules and non-standard shifts. While the methodology estimates income based on a typical clinical workday to establish standardized hourly rates for each specialty group, it does not require physicians to work those standard hours in practice.
Instead, the model supports a consistent hourly rate to be applied to the actual hours worked or funded within a program, allowing physicians working shorter or non-standard shifts to be compensated proportionately
The family medicine (FM) rate was developed using the existing economic section structure used in the allocation process, which does not differentiate between FM subspecialties.
FM physicians with enhanced skills (e.g., emergency medicine, anesthesia, addiction medicine, etc.) are grouped together for rate-setting purposes. The grouping does not reflect CPSA certification categories or additional qualifications, such as CFPC Certificates of Added Competence (CAC).
The AMA acknowledges that the inability to distinguish these subspecialties within the economic section of FM is a concern for many practices, sections and physicians. As this issue affects both ARPs and FFS, it requires further discussion and negotiations with PPHS.
The DDA methodology determines a daily base rate using FFS payments and excludes ARP claims data; the PCPCM model is an ARP.
As payment models evolve and affect physician compensation, the DDA will need to support integration of applicable components from other compensation models to ensure fairness and alignment with other provincial solutions.
After-hours time premiums are not included in the base cARP rate calculation. Instead, physicians in eligible programs can bill the 03.01AA premium for regularly scheduled after-hours services with payments provided on top of the program’s base cARP funding. LEARN MORE
While there is no formal appeal mechanism, physicians can share questions or provide feedback by contacting [email protected].
Background: The AMA collaborated with PPHS to establish the methodology and in November 2024, an engagement session took place with AMA physician leaders from each economic section, ARP representatives and AMHSP representatives. The session was an opportunity to provide input into the proposed methodology and rates and feedback informed subsequent recommendations that the AMA brought forward to the joint ARP Working Group.
Additional engagement sessions were held throughout 2025 to provide updates and seek final input from section leaders, fees representatives, ARP representatives and AMHSP representatives.