
Contributed By: Serena Rix (PharmD, MSc [Palliative Care]) – View bio
Case
Jane is a 75-year-old woman with end-stage colon cancer, metastatic to the liver and lungs. She is currently admitted to an acute care facility for symptom control, including neuropathic pain, malignant bowel obstruction, agitation, dyspnea, nausea and vomiting. She has a venting PEG tube in place and a C1 goals-of-care designation (comfort-focused care). Her prognosis is estimated to be weeks.
Jane is a retired nurse who was widowed five years ago and is capable of making her own decisions. She has one child, Karen, who lives in Texas and is a journalist for the local newspaper. Karen is designated as Jane’s primary decision-maker (PD) and power of attorney (POA).
Jane’s current medications include:
- methadone 10 mg subcut q8h and 5 mg subcut q1h PRN for pain/dyspnea
- dexamethasone 4 mg subcut in the morning and at noon
- fentanyl 100 mcg subcut q1h for care/turns
- octreotide 200 mcg subcut q8h
- haloperidol 1 mg subcut q6h and q1h PRN for agitation, restlessness, nausea or vomiting
- methotrimeprazine 12.5 mg subcut q1h PRN if haloperidol is ineffective
- sodium chloride 0.9% subcut at 30 mL/h
The palliative team is following Jane, and she has requested palliative sedation with midazolam if the dyspnea becomes refractory.
Karen has been updated about her mother’s condition and will be arriving tomorrow. She has been fact-checking online and has discovered that “methadone is for drug addicts, fentanyl kills people, haloperidol is for psychosis and methotrimeprazine is not used in the US.” Karen is outraged at what she perceives is inappropriate prescribing and wishes to move her mother to Texas for “strong chemotherapy and proper care.”
At first glance, Karen may have a point; however, a deeper dive into the case reveals most of these medications are being used off-label. Is this responsible prescribing?
Evidence
Off-label prescribing (OLP) is defined as the use of a licensed medication outside of marketing authorization.1 The label identifies indications, directions, patient population and routes of administration. It also includes safety information and the product monograph, which may vary depending on the licensing authority (e.g., Health Canada, FDA in the US or EMA in the European Union).1, 2
Prescribing outside any of these parameters is considered OLP. A study from Quebec suggested 11% of prescriptions for seniors were used off-label, and 79% of these lacked strong supporting evidence.3 Good evidence may include randomized controlled trials, licensure in other jurisdictions or prescriber expertise and experience.2
As the geriatric population is underrepresented in clinical trials, it is not surprising that OLP rates are higher in this group.4 Clinical trials are costly and time-consuming, so there is little financial incentive to initiate new studies on existing medications, particularly older drugs that no longer have patent protection and therefore offer little commercial return.2
In practice, formulary coverage and cost also influence off-label prescribing. Many older medications commonly used off-label (e.g., haloperidol or methotrimeprazine) are inexpensive and widely available on hospital formularies, allowing prescribers to use them for a range of indications with minimal restriction. In contrast, higher-cost medications may have specific formulary criteria or require justification for off-label use, particularly in outpatient settings where coverage through drug benefit plans may be limited. Clinicians may therefore need to balance clinical benefit with cost, access and feasibility of administration.
Other studies suggest OLP may be as high as 75% in the pediatric population and 50% in palliative care patients.1, 2, 5, 6 Therefore, OLP may be clinically necessary to provide good patient care.
OLP should be patient-centred. Clinicians must determine whether the therapy is appropriate for the patient’s current condition, reassessing as circumstances change. Prescribing should also align with the patient’s values and expectations and may necessitate individual prescriber expertise.
Health care professionals may have concerns about prescribing off-label. Survey data suggests a desire for clearer regulatory guidance, including recommendations for management. Prescribers have also expressed interest in greater legal security and protection from bureaucratic prescribing.1, 7
“Bureaucratic prescribing” refers to situations where restrictive formularies or coverage criteria limit a clinician’s ability to select what they believe is the most appropriate therapy. While these structures are intended to support safe and cost-effective care, they can create challenges when the best option for a patient falls outside standard indications or funding criteria. In such cases, prescribers may need to pursue non-formulary requests, provide supporting evidence or consider alternative approaches based on access and feasibility.
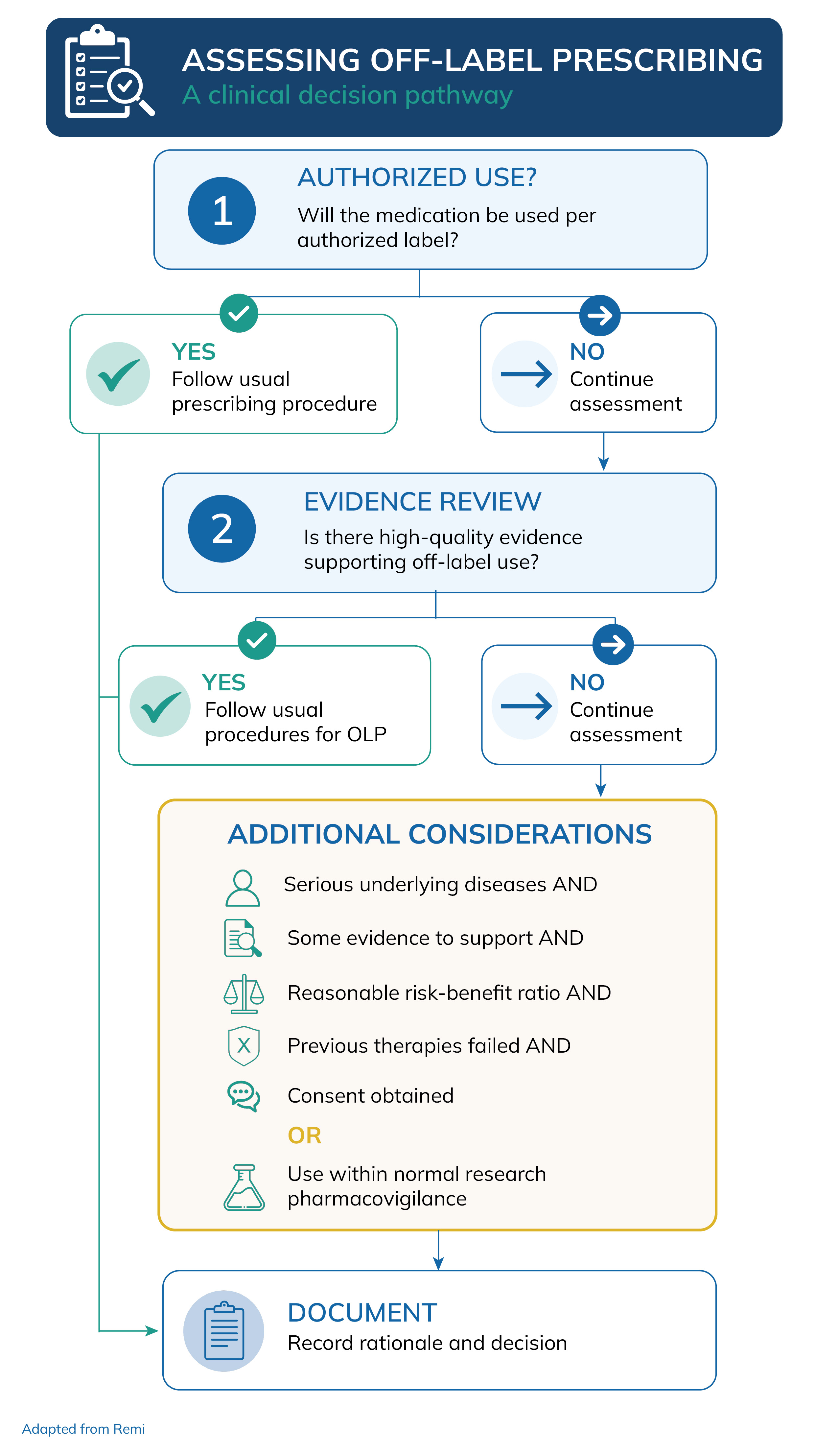
If you think your patient would benefit from off-label prescribing, consider the following:
Requirements for OLP
- Approved alternatives are inappropriate or have been tried and failed.
- There is a reasonable expectation for therapeutic benefit.
- There is evidence of a scientifically demonstrated effect.
- The risk of complications is low and there is evidence to suggest it is safe.1, 2
If the patient meets the requirements for OLP, follow the steps outlined below.
Together, these criteria align with regulatory expectations, which emphasize informed consent, evidence-based rationale and appropriate documentation when prescribing off-label.
Steps for OLP
- Identify which medication is to be used off-label.
- Explore current medical standards and consider alternatives.
- Obtain informed consent and outline treatment expectations.
- Ensure documentation in the chart includes:
- Name of the medication, dose and indication
- List of failed treatments
- Confirmation that informed consent was obtained
- Treatment expectations (expected effects, goals of care and when to stop)
- Monitoring plan, including toxicity, efficacy, cost-effectiveness and alignment with applicable formulary or institutional policies.1
Resolution of case
A family meeting was arranged when Karen arrived. Jane, Karen and the care team were present, and Jane consented to share medical information with Karen.
The team explained that Jane is in a palliative stage and remains capable of making her own decisions. Chemotherapy has been offered, but she declined, opting instead for a comfort-focused approach. Jane is aware that many of her medications are being used off-label and that the palliative care team has experience using them effectively to manage end-of-life symptoms.
Jane states that her symptoms have improved significantly with the current treatment and that she is willing to accept potential risks.
During the conversation, Karen comes to understand that Jane has carefully considered her options and that her rationale for selecting comfort-focused care is sound and aligns with her values. Jane recognizes that palliative practitioners often use medications off-label to optimize symptom control and quality of life, which may also be associated with improved survival compared with more aggressive care.8,9
By the end of the meeting, Karen accepts her mother’s decision and agrees to support her in the difficult days ahead.
References
1. Remi CE, Bausewein CE. Off-label use in Palliative Medicine Munich, Germany 2020. Available from: www.palliativmedizin.de.
2. Canadian Agency for Drugs and Technologies in Health (CADTH). Off-label use of drugs. Questions and answers about off-label use of drugs for health care providers. 2017. Available from: https://canadacommons.ca/artifacts/34190066/off-label-use-of-medications/35089713/.
3. Bernier NF. Improving prescription drug safety for Canada Seniors IRPP Study No. 61; 2017. Available from: https://irpp.org/research-studies/improving-prescription-drug-safety-for-canadian-seniors/.
4. Jackson SH, Jansen PA, Mangoin AA. Off-label prescribing in older patients. Drugs Aging. 2012;29(6):427-34.
5. Hagemann V, Bausewein C, Remi C. Off-label use in Palliative Care - more common than expected. A retrospective chart review. European Journal of Hospital Pharmacy. 2022;6:329-35.
6. Kwon JH, Kim MJ, Bruera S, Park M, Bruera E, Hui D. Off-label medication use in the inpatient palliative care unit. Journal of Pain and Symptom Management. 2017;54(1):46-54.
7. Wernli U, Durr F, Jean-Petit-Matile S, Kobleder A, Meyer-Massetti C. Subcutaneous drugs and off-label use in hospice and palliative care: a scoping review. Journal of Pain and Symptom Management. 2022;64(5):e250-e9.
8. Delisle ME, Ward MA, Helewa RM, Hochman D, Park J, McKay A. Timing of palliative care in colorectal cancer patients: Does it matter? Oncology. 2019;241:285-93.
9. Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, Jackson VA, et al. Early palliative care for patients with metastatic non-small cell lung cancer. New England Journal of Medicine. 2010;363(8):733-42.
