Background:
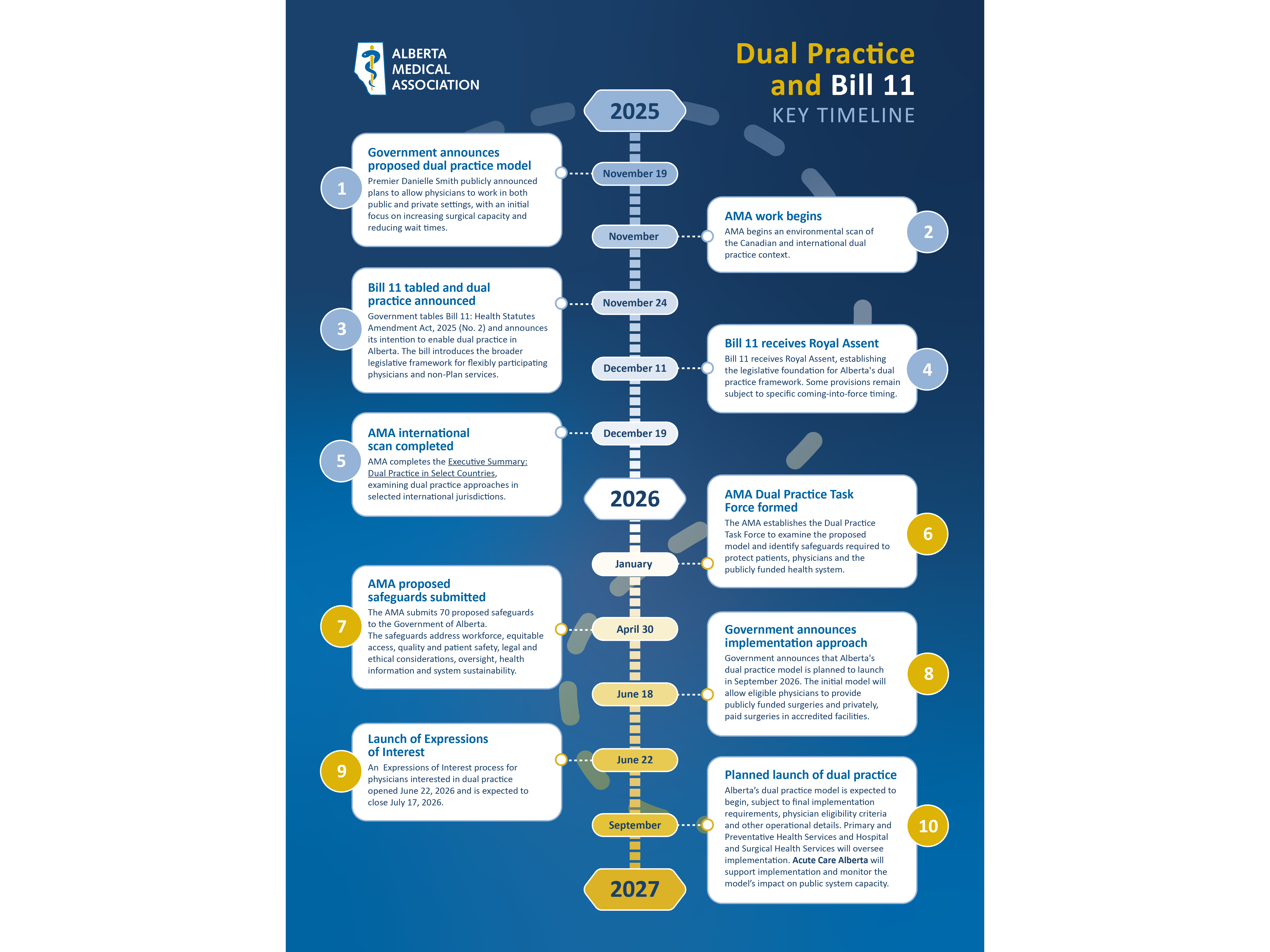
On November 19, 2025, the Alberta government announced a Dual Practice Surgery model that would let surgeons perform elective surgeries in both the public and private systems on the condition they commit to doing a certain number of publicly funded operations.
Bill 11, the Health Statutes Amendment Act, 2025 (No. 2), received Royal Assent in December 2025. It amended Alberta’s health legislation to create new physician participation categories and enable eligible physicians to provide both publicly funded and privately paid non-Plan services.
On June 18, 2026, Minister of Hospital and Surgical Health Services, Adriana LaGrange announced a Dual Practice Surgery model will be rolled out across Alberta in September, with eligible physicians being able to express interest beginning June 22.
Dual practice:
Dual practice generally refers to physicians working in both publicly funded and privately paid care. Under Alberta’s proposed model, some physicians could continue providing insured services through the public system while also providing designated services that patients pay for privately. The specific services, participation requirements and operational rules are established through legislation, regulations and government policy.
The Government of Alberta has described dual practice as a way to:
- Expand surgical and procedural capacity
- Reduce wait times
- Provide physicians with greater practice flexibility
- Support physician recruitment and retention
- Give patients more choice while maintaining access to publicly funded care
Government has stated that publicly insured services will remain available without out-of-pocket charges and that private services will operate in defined and monitored circumstances.
The AMA’s position:
The AMA has emphasized that significant health system reform should be evidence-informed, transparent and developed with meaningful physician and patient involvement. We have not framed our work as simply supporting or opposing dual practice.
Our focus has been on ensuring that, should the model proceed, it:
- Protects access based on clinical need rather than ability to pay.
- Does not destabilize publicly funded care.
- Protects patient safety and continuity of care.
- Supports health workforce sustainability.
- Includes clear accountability and oversight.
- Is supported by practical, enforceable safeguards.
The AMA’s position is that dual practice must not:
- Displace or delay publicly funded care.
- Divert scarce health workforce from public services.
- Create preferential access based on ability to pay.
- Transfer private-sector risks or costs to the public system.
- Undermine patient safety, continuity of care or public trust.