
The panel payment component of the Primary Care Physician Compensation Model (PCPCM) recognizes the continuous relationship between a family physician and their patient and acknowledges increased demands placed on physician practices by complex patients.
Panel payments for PCPCM are determined by the number of patients attached to a family physician’s PCPCM panel (derived from CPAR) and which cell within the complexity matrix the patients fit within. Scroll down or click here for a calculation guide.
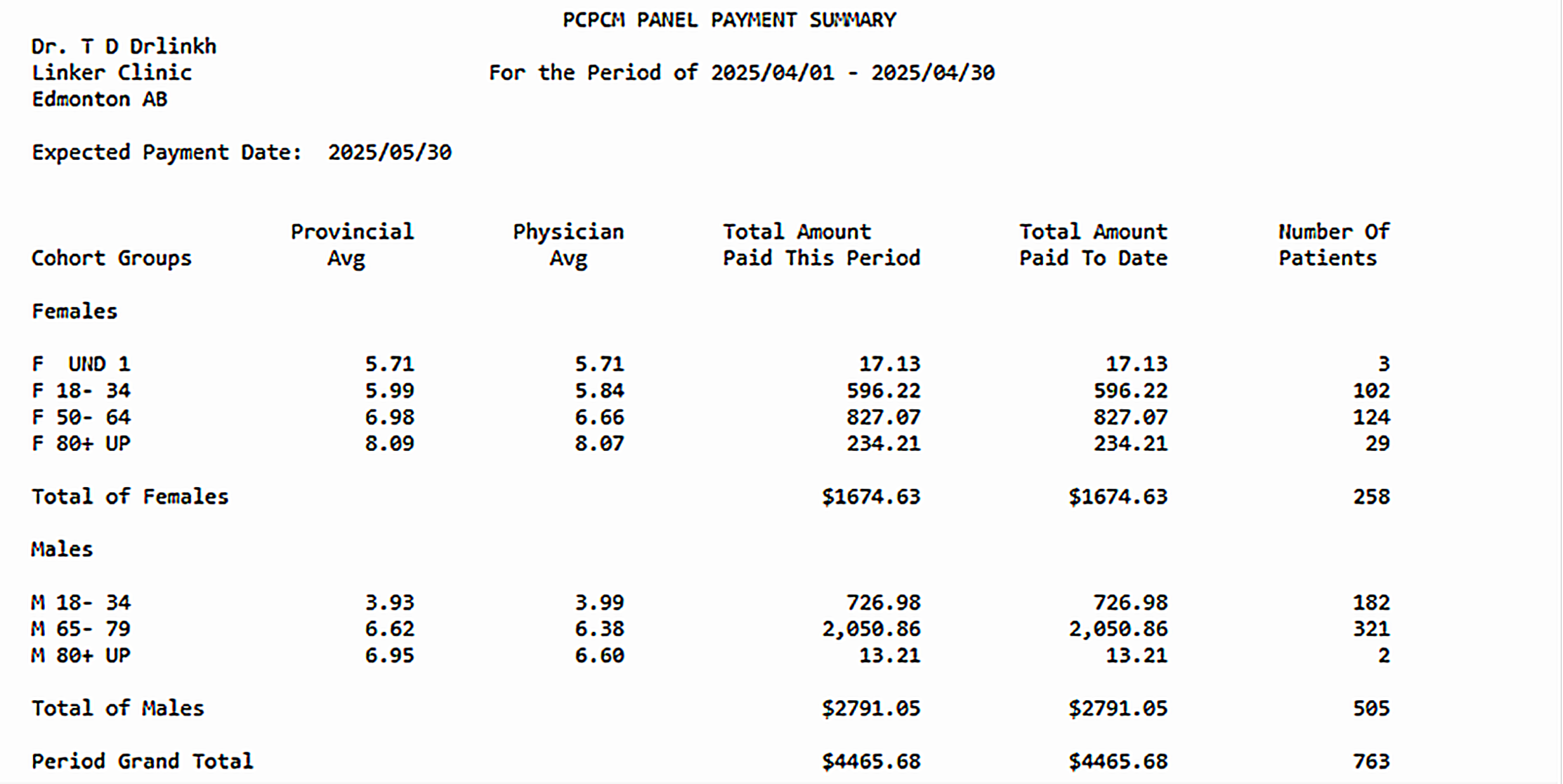
New for PCPCM Physicians: Panel payment details can be found through a monthly report shared by Primary & Preventative Health Services (PPHS). See example of the PC001 Report below.
PC001 Report Example
New for PCPCM Physicians: To support ongoing panel monitoring (to maintain the minimum number of patients required to stay on the model), physicians or their panel administrator can access a new Panel Submissions Metric report in the CPAR portal.
Complexity-Adjusted Panel Payments Calculation Guide
This guide offers PCPCM physicians and those interested in the model with an outline of how Complexity-Adjusted Panel Payments are calculated.
1: Complexity Categories
All Alberta residents are assigned to a complexity category using the Canadian Institute for Health Information Population Grouping Methodology (CIHI Pop Grouper). PPHS runs CIHI’s program using multiple data sources containing demographics and health care data.
Health Care Data Sources
-
Physician claims
-
Ambulatory care
-
Inpatient
-
Home care
-
Long-term care
Types of Data Utilized
-
Medical diagnoses (ICD-9 and ICD-10)
-
Healthcare system usage
-
Age
-
Gender
Alberta residents are placed in one of seventeen complexity categories:
- Healthy newborn
- Major acute
- Major cancer
- Major chronic
- Major mental health
- Major newborn
- Minor acute
- Minor chronic
- Moderate acute
- Moderate chronic
- Non-users
- Obstetrics
- Other cancer
- Other mental health
- Palliative
- Users without health conditions
- Unassigned
The last category of “Unassigned” is for residents with insufficient data for classification.
2: Age and Gender
PPHS further separates residents by age and gender to create a complexity-adjusted payment matrix.
Gender Categories
-
Female
-
Male
-
Unknown or Other - categorized as Male
Age groups: 0-1, 1-17, 18-34, 35-49, 50-64, 65-79, and 80+.
3: Payment Calculation Matrix
Once patients are assigned to a cell within the matrix, the funding value of the cell is determined. PPHS uses the total cost of primary care physician visits and divides that by the number of residents in that cell to create an average cost per patient.
Example Assignment: Major Acute – Female - 18-34

When calculating the PCPCM payment, it uses a proportion of the Blended Capitation Model (BCM) where the average patient rate is $306.60. In PCPCM, the average patient is currently paid at $70.25 per patient, which is 22.9% of the average rate for BCM.
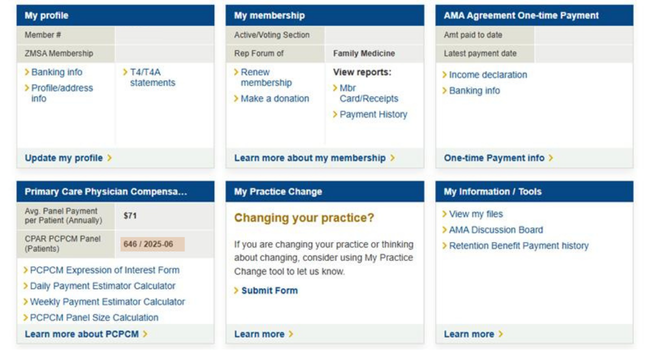
In the AMA Member Portal, non-PCPCM physicians can view their CPAR PCPCM Panel calculation and Average Panel Complexity Payment per Patient data. Physicians who are already on the model will not see updates to their data. See screenshot below.
4: Adjusting for Funding Increases
To account for funding increases in the Alberta Medical Association’s SFM agreement with PPHS, the values from Step 3 sometimes need to be adjusted, as they reflect the cost values from prior years.
Macro-allocation rate increases are calculated by multiplying the prior year’s value by the rate increase. For example, if the SFM were to receive a 5% increase in the future, here's the adjusted rate:
[Previous Year Avg Cost $] X [Current Year % Rate Increase] = Adjusted Rate
$70.25 X 1.05 = $73.76
Schedule 3
2022/23, 2023/24 & 2024/25 Macro-Allocations
|
AMA Member Section |
Year 1 (2022/23) Rate Increase |
Year 1 BCP Increase Estimate |
Year 2 (2023/24) Rate Increase |
Year 3 (2024/25) Rate Increase |
Compounded Increase First Three Fiscal Years |
|
Family Medicine & Generalists in Mental Health |
1.35% |
0.89% |
1.48% |
1.48% |
5.25% |
Source: AHCIP Bulletin MED 280
Fee for Service Retroactive Payments for 2024-25 Fiscal Year
Note: AMA physician leaders are confident that CIHI is a transparent and appropriate methodology to use for PCPCM. CIHI works with all 13 provinces and territories, as well as the federal government, to support evidence-based decision-making in healthcare. Other options for panel complexity calculations were explored, and the CIHI methodology was determined to be the most appropriate option.
CPAR Conflicts & PCPCM Panel Payments
Starting in April 2026, PCPCM physicians may see changes to their panel payment calculation. Patients in conflict with other providers may be subtracted from the monthly payment calculation.
Physicians should work with their teams to implement a structured, ongoing Conflict management process. Get started here.
More Resources
- Watch a short video on the Population Grouping Methodology
- The Ontario Medical Association has learning modules on CIHI’s Population Grouping Methodology. To request this resource, please email [email protected]